
+
JMJ
I may have had a subsequent bout of covid this past week. Why do I think that? Well my mom, who I visited last week, developed symptoms at the same time as I did. At first I thought my allergies had upped their game as I was having difficulty breathing and a long cough. Now I'm not so sure. What I do know is that my mom has covid and whatever I had made it difficult to breathe.
Not a sensation that I wish to repeat.
Now to stir the pot ...
This article ( Ivermectin for COVID-19: Final Nail in the Coffin) popped up in one my news feeds and I thought I would give it a read. While I have friends who took Ivermectin and believe it helped them with Covid or even prevented it, I typically find the studies that show a lack of significant response reliable and the belief that Ivermectrin prevented covid as being hard to prove.
Jumping back to the root of the Ivermectin story, the medscape article notes the following:
Ivermectin, a widely available, cheap, and well-tolerated drug on the WHO's list of essential medicines for its critical role in treating river blindness, was shown to dramatically reduce the proliferation of SARS-CoV-2 virus in cell culture. You know the rest of the story. Despite the fact that the median inhibitory concentration in cell culture is about 100-fold higher than what one can achieve with oral dosing in humans, anecdotal reports of miraculous cures proliferated.
Once panicked people get a hold of a story, just like conspiracy theories, they take on a life of their own. The author even wrote this comment:
And every time a study came out that seemed like the nail in the coffin for the so-called horse paste, it rose again, vampire-like, feasting on the blood of social media outrage.
The author highlights two studies - one in Brazil (Together Trial) and one in the states (Activ-6). The Brazil trials showed no significant difference between placebo and Ivermectin.
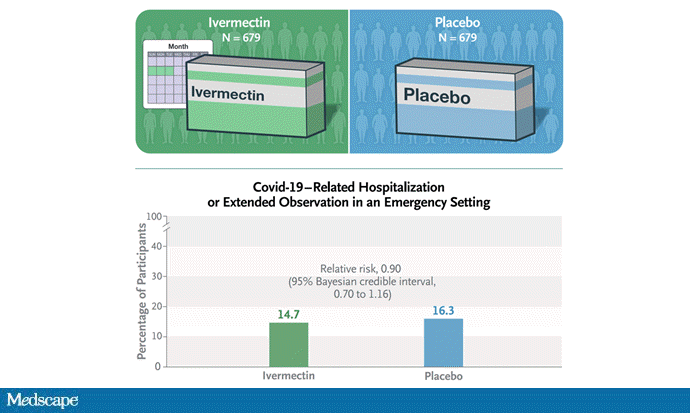
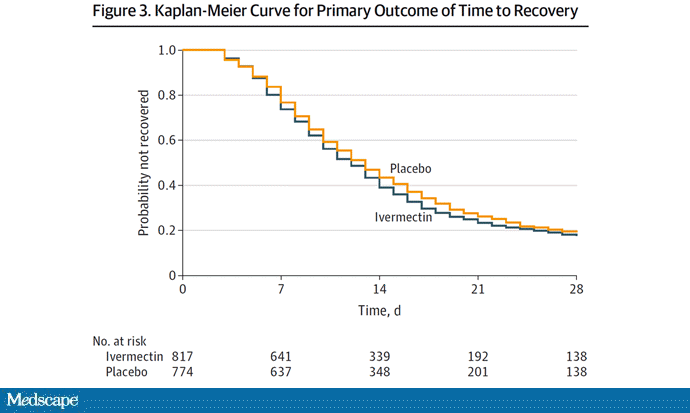
The Activ-6 paper can be found here (link) and it concluded:
Conclusions and Relevance Among outpatients with mild to moderate COVID-19, treatment with ivermectin, compared with placebo, did not significantly improve time to recovery. These findings do not support the use of ivermectin in patients with mild to moderate COVID-19.So, while a Doctor may prescribe Ivermectin, there isn't any proof that it will cure, prevent or alter the outcomes in a significant manner. By the way, self medicating with Ivermectin is obviously not recommended - especially with Veterinary source pharmaceuticals.
But overall, everyone in the trial did fairly well. Serious outcomes, like death, hospitalization, urgent care, or ER visits, occurred in 32 people in the ivermectin group and 28 in the placebo group. Death itself was rare — just one occurred in the trial, in someone receiving ivermectin.Here's the graph showing the results:
One possible point of contention are the cohort studies noted in the Medscape article.
Cohort studies suggested that people who got ivermectin did very well in terms of COVID outcomes.
So me being me, I went to look at the cohort study. Here's the summary of the findings:
- Study Question: Is ivermectin associated with lower mortality rate in patients hospitalized with coronavirus disease 2019 (COVID-19)?
- Results: A retrospective cohort study of consecutive patients hospitalized with confirmed severe acute respiratory syndrome coronavirus 2 infection at a four-hospital consortium in South Florida. Analysis showed statistically significant lower mortality rates in the group treated with ivermectin as compared with the group treated with usual care (15.0% vs 25.2%).
- Interpretation: Ivermectin was associated with lower mortality during treatment of COVID-19 patients, especially in patients who required higher inspired oxygen or ventilatory support.
If you stop reading at this point ... all looks good for the Ivermectin conspiracy theory. Then there's this:
Randomized controlled trials are needed to confirm these findings.
The difference is that this study was a cohort study, as opposed to a randomized controlled study.
Cohort Study:
Cohort studies differ from clinical trials in that no intervention, treatment, or exposure is administered to participants in a cohort design; and no control group is defined. ... Exposures or protective factors are identified as preexisting characteristics of participants. The study is controlled by including other common characteristics of the cohort in the statistical analysis. Both exposure/treatment and control variables are measured at baseline. Participants are then followed over time to observe the incidence rate of the disease or outcome in question. Regression analysis can then be used to evaluate the extent to which the exposure or treatment variable contributes to the incidence of the disease, while accounting for other variables that may be at play.(Source: Wikipedia)
Randomized Controlled study:
Double-blind randomized controlled trials (RCTs) are generally considered superior methodology in the hierarchy of evidence in treatment, because they allow for the most control over other variables that could affect the outcome, and the randomization and blinding processes reduce bias in the study design. This minimizes the chance that results will be influenced by confounding variables, particularly ones that are unknown. However, educated hypotheses based on prior research and background knowledge are used to select variables to be included in the regression model for cohort studies, and statistical methods can be used to identify and account potential confounders from these variables. Bias can also be mitigated in a cohort study when selecting participants for the cohort. It is also important to note that RCTs may not be suitable in all cases; such as when the outcome is a negative health effect and the exposure is hypothesized to be a risk factor for the outcome. Ethical standards, and morality, would prevent the use of risk factors in RCTs. The natural or incidental exposure to these risk factors (e.g. time spent in the sun), or self-administered exposure (e.g. smoking), can be measured without subjecting participants to risk factors outside of their individual lifestyles, habits, and choices. (Source: Wikipedia)Anyway, I'm confident that the Ivermectin story will eventually go the same was as the Hydroxychloroquine story. There will remain the adherents, who believe themselves instead of Pope Emeritus B16 on whether we have to acknowlege that Pope Francis is the totally worthless Vicar of Christ in a long time.
P^3
P^3
Comments
Post a Comment